Blood glucose concentration must be maintained within narrow limits — too high or too low is dangerous.
Why does blood glucose need to be controlled?
Why does blood glucose need to be controlled?
- Too high — lowers the water potential of the blood. This can cause water to move out of cells by osmosis, potentially damaging them.
- Too low — cells don’t have enough glucose for respiration, so they can’t produce sufficient ATP for energy-requiring processes.
This is an example of homeostasis regulated by hormones secreted from the islets of Langerhans in the pancreas.
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
- What raises and lowers blood glucose concentration
- How the liver regulates blood glucose through glycogenesis, glycogenolysis and gluconeogenesis
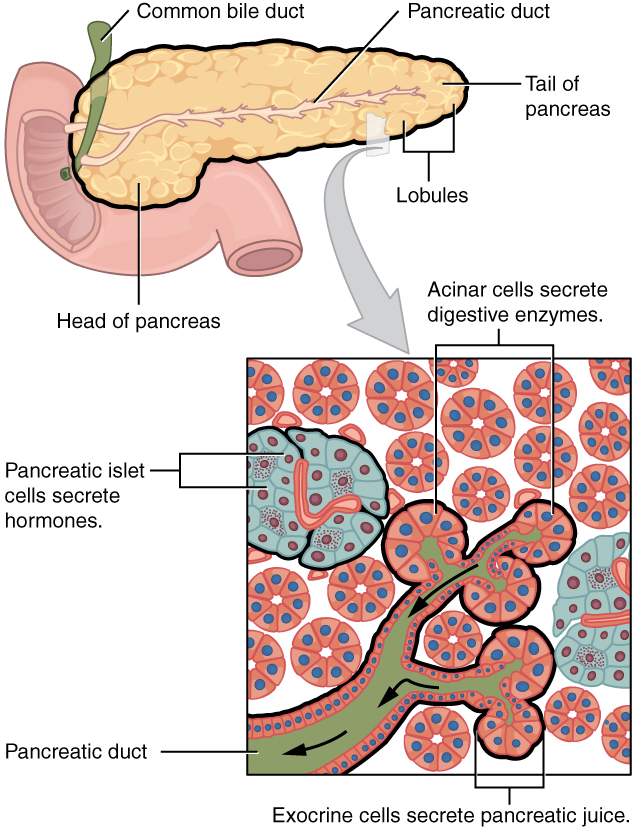
The Pancreas & Islets of Langerhans
The islets of Langerhans are clusters of hormone-secreting cells scattered throughout the pancreas:
| Cell type | Hormone secreted | Response to… |
|---|---|---|
| Alpha (α) cells | Glucagon | Low blood glucose |
| Beta (β) cells | Insulin | High blood glucose |
{kind=link}
Tip
Don’t confuse the islets of Langerhans (endocrine — secrete hormones into blood) with the acinar cells of the pancreas (exocrine — secrete digestive enzymes into the gut).
Genesis & Lysis
Key phrases you need to understand:
-
Glycogenolysis
- Breakdown of glycogen to glucose (when blood glucose levels are too low)
- Liver & muscle cells
-
Glycogenesis
- Synthesis of glycogen from glucose (when blood glucose levels are too high)
- Removes glucose from the bloodstream by converting it to glycogen (a storage molecule)
- Liver & muscle cells
-
Gluconeogenesis
- Synthesis of glucose from non-carbohydrate molecules (e.g. amino acids, glycerol)
Tip
Think about the word: genesis = creation, lysis = splitting/breaking down. So glycogenesis = creation of glycogen. Glycogenolysis = breaking down of glycogen.
High Blood Glucose → Insulin (Beta Cells)
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
How insulin lowers blood glucose:
- Binds to specific receptors on the cell surface membrane of target cells
- Increases glucose uptake by stimulating insertion of GLUT4 glucose transporter proteins into cell surface membranes
- Activates enzymes that convert glucose to glycogen (glycogenesis)
When blood glucose rises (e.g. after a meal):
-
Beta cells detect the rise and secrete insulin into the blood
-
Insulin binds to specific receptors on the cell surface membrane of target cells e.g. liver, muscle, and adipose cells. Insulin has a complementary shape to the insulin receptor. Anything that changes the amino acid sequence of insulin (e.g. neonatal diabetes) means that the tertiary structure of insulin is changed, and it is no longer complementary to the insulin receptor.
-
Insulin triggers movement and fusion of vesicles containing glucose transporter proteins (GLUT4) with the cell membrane, increasing the number of glucose transporter (GLUT4) carrier proteins → more glucose enters the cell by facilitated diffusion, removing glucose from the bloodstream
-
Insulin also activates enzymes for glycogenesis which convert glucose → glycogen

As a result of the above changes, this causes:
- Increased rate of absorption of glucose into cells (muscle cells especially)
- Increased rate of cellular respiration — more glucose is available inside the cells (via GLUT4), so more substrate is available for respiration
- Increased conversion of glucose to glycogen
Low Blood Glucose → Glucagon (Alpha Cells)
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
How glucagon raises blood glucose:
- Binds to receptors on the cell surface membrane of target cells (primarily liver cells)
- Activates enzymes that break down glycogen into glucose (glycogenolysis)
- Activates enzymes that synthesise glucose from non-carbohydrate precursors — glycerol and amino acids (gluconeogenesis)
When blood glucose falls (e.g. between meals, during exercise):
-
Alpha cells detect the fall and secrete glucagon into the blood
-
Glucagon binds to receptors on target cells (main target is liver cells)
-
Acts via the second messenger model (see below)
-
Activates glycogenolysis — enzymes break down glycogen → glucose, released into blood
-
Activates gluconeogenesis — glucose synthesised from non-carbohydrate precursors:
- Glycerol
- Amino acids (from protein breakdown)

Tip
Glycerol not fatty acids are used in gluconeogenesis
Adrenaline (Fight or Flight)
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
How adrenaline raises blood glucose:
- Binds to receptors on the cell surface membranes of target cells (liver and muscle)
- Activates enzymes that convert glycogen to glucose (glycogenolysis)
Adrenaline is released from the adrenal medulla (adrenal glands) in response to stress or exercise — triggered by the nervous system, not blood glucose levels directly.
- Binds receptors on liver and muscle cells
- Activates glycogenolysis (glycogen → glucose)
- Inhibits glycogenesis
- Promotes glucagon secretion, inhibits insulin secretion
- Acts via the second messenger model (same cAMP pathway as glucagon)
Tip
Unlike insulin and glucagon, adrenaline responds to stress/fear/exercise via the nervous system — not directly to blood glucose concentration. It raises blood glucose as part of preparing the body for rapid action, regardless of current glucose levels.
Second Messenger Model (cAMP)
Glucagon and adrenaline both work via the second messenger model:
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
How glucagon and adrenaline act via the second messenger model — including the roles of adenylyl cyclase, cyclic AMP (cAMP) as the second messenger, and protein kinase A in amplifying the signal inside the cell.
- Hormone (glucagon/adrenaline) = first messenger — binds complementary receptor on cell surface membrane
- This causes the receptor to change shape inside the cell membrane. This activates the enzyme adenylyl cyclase
- Adenylyl cyclase converts ATP → cAMP (second messenger)
- cAMP activates protein kinase A
- Protein kinase A activates conversion of glycogen to glucose (glycogenolysis) and inhibits glycogenesis

Tip
The hormone is the first messenger, cAMP is the second messenger. The receptor is not the first messenger.
Diabetes
What you need to know (based on the AQA specification)
What you need to know (based on the AQA specification)
- The underlying causes of Type 1 and Type 2 diabetes and how each is managed through insulin therapy or dietary changes
- Be able to weigh up the roles of health professionals and the food industry in the rising prevalence of Type 2 diabetes
| Type 1 | Type 2 | |
|---|---|---|
| Cause | Autoimmune destruction of β cells | Insulin resistance (cells less responsive) |
| Insulin production | None | Reduced or normal but ineffective |
| Onset | Usually childhood/young adult | Usually adult onset |
| Treatment | Insulin injections | Diet, exercise, medication |
What does reduced insulin sensitivity mean?
What does reduced insulin sensitivity mean?
Target cells have fewer insulin receptors or the receptors are less responsive to insulin. This means even when insulin is present, cells don’t take up glucose as effectively — so blood glucose remains high.